The Return of the Flu
COVID19 - CORONAVIRUS, 29 Nov 2021
Swiss Policy Research - TRANSCEND Media Service
24 Nov 2021 – The flu has returned to some countries with high rates of natural immunity against SARS-CoV-2. In contrast, countries with high vaccination rates but low natural immunity rates are seeing record new covid waves, although at lower hospitalization and death rates than previously.
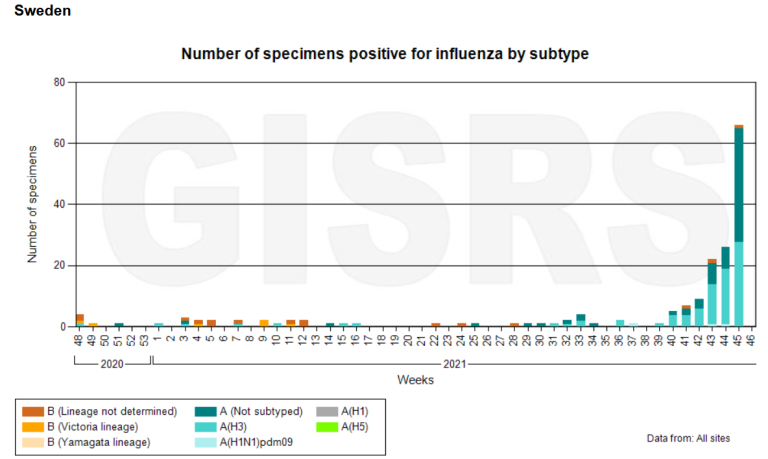
Sweden: The return of the flu (WHO FluNet)
In March 2020, shortly after the beginning of the coronavirus pandemic, influenza viruses and some other respiratory viruses mysteriously disappeared from global circulation. Some skeptics suspected that influenza was simply ‘rebranded’ as covid, while many health authorities and journalists claimed influenza was suppressed by face masks and lockdowns.
But influenza has not been rebranded as covid, and influenza viruses have disappeared even in countries without face masks and lockdowns (e.g. Sweden), while they did not disappear during previous flu pandemics, despite face masks, school closures, and other measures. In fact, face masks and most other measures simply aren’t effective against respiratory virus transmission.
Instead, influenza viruses have been displaced by the more infectious novel coronavirus. This “displacement effect” is well known from previous influenza pandemics (e.g. 1918, 1957 and 1968) and is at play every winter, when various respiratory viruses displace each other. Even during the ongoing coronavirus pandemic, new variants have repeatedly displaced previous variants. (1)
Thus, it was only a matter of time until influenza viruses would re-emerge somewhere, most likely at a place that had achieved a high rate of natural immunity against the novel coronavirus.
This moment came in July 2021, when the first major influenza wave since early 2020 hit India, shortly after its large Delta coronavirus wave had ended in June (see WHO flu chart below). At the time, the natural immunity rate in India was about 80% at the national level and about 97% in the capital city, Delhi, while the covid vaccination rate was only about 5%. (2)
More recently, influenza has also returned to Sweden (see chart above), which had achieved a natural immunity rate of about 60% by October and hasn’t yet seen a new coronavirus surge this winter. However, the current Swedish flu wave is still quite weak and may collapse at any time.
Indeed, in some other European countries, influenza briefly showed up in October but was again displaced by a new coronavirus wave in November (e.g. in the Netherlands). Some places in the United States have also seen local influenza waves recently, especially on university campuses.
Great Britain, meanwhile, has experienced a prolonged Delta wave since June and may have reached a total infection rate of about 50% (3). In the next few weeks, Great Britain might see either a renewed covid winter surge, or a collapse of the Delta wave followed by a flu surge. In South Africa, which experienced three consecutive strong covid waves of the Wuhan, Beta and Delta variants, influenza currently appears to be gaining the upper hand for the first time. (4)
In contrast, countries with a high covid vaccination rate but a rather low natural infection rate have not yet seen a return of influenza, but instead have experienced record new coronavirus waves. This was the case in Israel, Iceland, Singapore and in several Western European countries. Moreover, countries with some of the strictest “covid certificate” rules in the world, such as the Baltic states, have seen the highest coronavirus infection rates in the entire world.
Countries with very low infection rates, such as Australia, New Zealand, Norway, Finland and especially China, are bound to see major coronavirus waves as soon as they open their borders. Ideally, these countries will open the “flood gates” before vaccine protection in senior citizens has significantly waned, in order to minimize resulting covid hospitalizations and deaths.
While parallel coronavirus and influenza virus waves seem unlikely (given the competition between the two viruses), the Indian precedent indicates that many European countries, the UK and parts of the US might see an influenza wave in the second half of the winter, shortly after the ongoing coronavirus waves will have ended.
Already in September, WHO regional director for Europe, Dr. Hans Kluge, acknowledged that current covid vaccines cannot prevent virus transmission and, therefore, cannot end the pandemic. Moreover, it has become clear that covid vaccine protection lasts only about half a year, whereas natural immunity appears to be significantly more robust and durable: in most countries, recovered people account for just a fraction of a percent of new cases and hospitalizations. (5)
These limitations of covid vaccines invalidate the global strategy, advanced by billionaire vaccine investor Bill Gates back in April 2020, that the pandemic can only be ended by vaccinating the entire world. Moreover, these limitations invalidate the case for “vaccine passports”. In addition, donating vaccines to “developing countries” is not going to be effective, either, as most countries in Africa, Latin America and South East Asia have already achieved natural immunity rates of 60% to 80%.
Indeed, it looks like the major distinction is no longer between “vaccinated” and “unvaccinated” people (as many politicians suggest), but between recovered and non-recovered people; thus, ironically, the pandemic is increasingly turning into a “pandemic of the vaccinated”. Yet the long-term immunity of recovered people is mostly ignored or downplayed by authorities, possibly because it might challenge the global vaccination and vaccine passport strategy.
Nevertheless, covid vaccines do provide strong protection against severe disease for about half a year and, thus, may already have saved hundreds of thousands of lives in 2021.
Yet regardless of vaccination rates, it appears plausible that the entire global population will get infected by the novel coronavirus within about three years. This raises the most important question of what impact covid vaccines will likely have on this process:
- In the best case, covid vaccines will mitigate the impact of initial infections in high-risk groups while not interfering with the subsequent build-up of durable natural immunity. For instance, it has been argued that vaccination campaigns during the 1957 and 1968 flu pandemics may have saved hundreds of thousands of lives in the US and in Europe.
- In a neutral case, covid vaccines will simply delay initial infections by a few months, but will not mitigate infections once they occur. This was the result of a recent British study, which found that in senior citizens, covid vaccines may have little effect beyond delaying infection.
- In the worst case, covid vaccines will, over time, aggravate subsequent infections by causing an effect called original antigenic sin (OAS) or even antibody-dependent disease enhancement (ADE). For instance, it has been known for many months that vaccinated people show a limited antibody response once infected (they don’t develop anti-N antibodies), and molecular simulation studies indicate that future coronavirus variants might potentially trigger ADE. (6)
Due to the limited duration of covid vaccine trials, it is impossible to know which of these scenarios will materialize. Thanks to their short-term protective effect, covid vaccines may have saved hundreds of thousands of lives in 2021, but their long-term impact remains more uncertain. In particular, an immune-escaping coronavirus variant might fundamentally change the outlook.
See also: WHO FluNet (WHO), CoVariants, and Covid vs. the flu (SPR)
Notes:
(1) Importantly, almost 90 years after the discovery of influenza virus (in 1933), this viral interference and displacement effect – and large-scale respiratory virus transmission and seasonality in general – is still not understood scientifically. This is why the epidemiology of respiratory viruses is still a rather pre-scientific field that has failed badly during the coronavirus pandemic.
(2) Of note, India suffered a total pandemic excess mortality of about 4 million deaths, or close to 50% compared to about 9 million deaths per year in a population of about 1.3 billion.
(3) British blood donor data indicates a natural infection prevalence – measured by anti-N antibodies – of only 10% to 30% (decreasing with age). However, it has been shown that vaccinated people no longer develop anti-N antibodies once infected (as the vaccine induces anti-S antibodies), so data from vaccinated blood donors underestimates true infection prevalence.
(4) In many Latin American countries, the Delta wave has ended in late October. Despite some of the highest infection rates in the world, Latin America – with the partial exception of Mexico – has not yet seen a resurgence of influenza, perhaps due to seasonality.
(5) Current serological studies estimate that a previous infection will protect against re-infection for about 2 years on average (or more) and against severe disease for several years at least. In contrast to vaccinated people, recovered people generally develop mucosal immunity, too.
(6) The fact that vaccinated people don’t develop anti-N antibodies once infected was to be expected (as vaccination induces neutralizing anti-S antibodies). The same response is seen in children and in some people with very mild covid, so this is not necessarily a negative effect. Yet it remains unknown how vaccinated people will respond to future coronavirus variants.
Figures
1) The Indian flu wave from July to October 2021
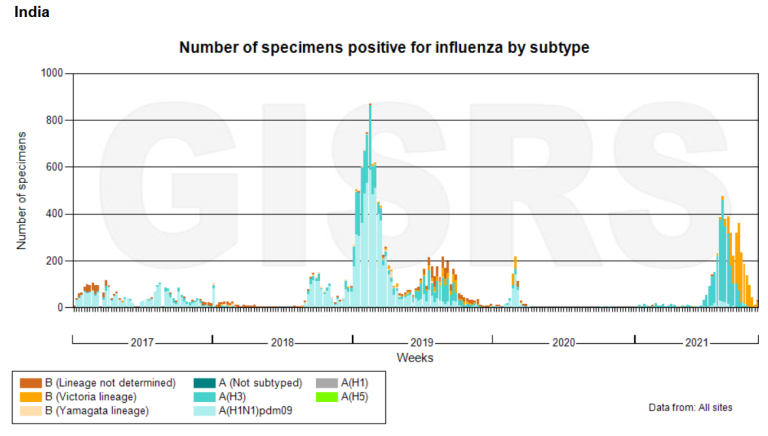
Flu waves in India (WHO FluNet)
2) Sweden vs. Japan: Disappearance of the flu
The flu disappeared both in Sweden (no lockdown, almost no masks) and in Japan (no lockdown, but high mask compliance). Moreover, in many countries, the flu disappeared several weeks prior to lockdowns and mask mandates. Chart: IanMsc
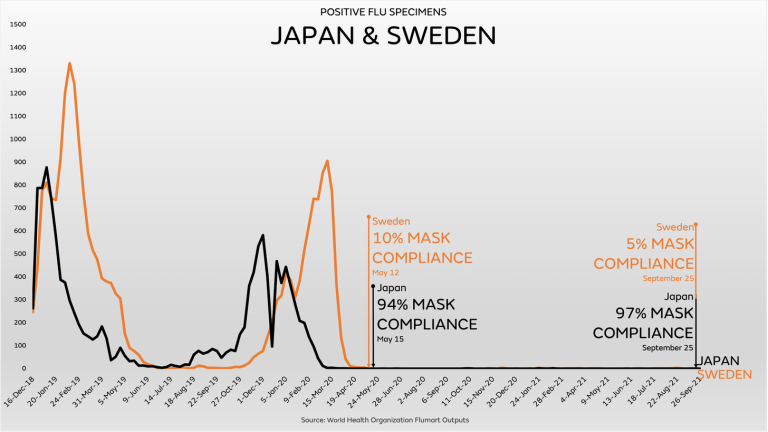
Disappearance of the flu in Sweden and Japan (IanMsc)
3) Competition between various respiratory viruses
Temporal patterns of seasonal respiratory viral infections in Glasgow (UK). Red: rhinoviruses, orange and yellow: influenza viruses, light green: coronaviruses, dark green: RS viruses.
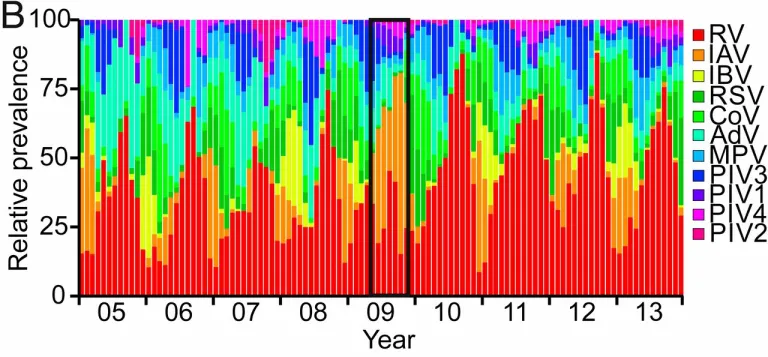
Temporal patterns of viral respiratory infections (Nickbaksh et al, 2019)
4) Timeline of pandemic influenza viruses

5) Coronavirus vs. influenza virus
Coronavirus vs. influenza virus (PN)
See also
__________________________________________
![]() Swiss Policy Research, founded in 2016, is an independent, nonpartisan and nonprofit research group investigating geopolitical propaganda in Swiss and international media. SPR is composed of independent academics that for personal and professional reasons prefer to protect their identities, and receives no external funding; there are no financial sponsors or backers. Our articles have been published or shared by numerous independent media outlets and journalists, among them Julian Assange, and have been translated into more than two dozen languages.
Swiss Policy Research, founded in 2016, is an independent, nonpartisan and nonprofit research group investigating geopolitical propaganda in Swiss and international media. SPR is composed of independent academics that for personal and professional reasons prefer to protect their identities, and receives no external funding; there are no financial sponsors or backers. Our articles have been published or shared by numerous independent media outlets and journalists, among them Julian Assange, and have been translated into more than two dozen languages.
Tags: COVID-19, Coronavirus, Flu, Influenza, Vaccines
DISCLAIMER: The statements, views and opinions expressed in pieces republished here are solely those of the authors and do not necessarily represent those of TMS. In accordance with title 17 U.S.C. section 107, this material is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. TMS has no affiliation whatsoever with the originator of this article nor is TMS endorsed or sponsored by the originator. “GO TO ORIGINAL” links are provided as a convenience to our readers and allow for verification of authenticity. However, as originating pages are often updated by their originating host sites, the versions posted may not match the versions our readers view when clicking the “GO TO ORIGINAL” links. This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more information go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
Read more
Click here to go to the current weekly digest or pick another article:
COVID19 - CORONAVIRUS: